This is “Understanding Daily Reference Intakes”, section 2.6 from the book An Introduction to Nutrition (v. 1.0). For details on it (including licensing), click here.
For more information on the source of this book, or why it is available for free, please see the project's home page. You can browse or download additional books there. To download a .zip file containing this book to use offline, simply click here.



2.6 Understanding Daily Reference Intakes
Learning Objective
- Use the Dietary Reference Intakes to determine daily nutrient recommendations.
Dietary Reference Intakes (DRI)A set of nutrient recommendations that includes the Estimated Average Requirements (EAR), Recommended Dietary Allowances (RDA), Adequate Intakes (AI), Tolerable Upper Intake Levels (UL) and Acceptable Macronutrient Distribution Range (AMDR). are the recommendation levels for specific nutrients and consist of a number of different types of recommendations. This DRI system is used in both the United States and Canada.
Daily Reference Intakes: A Brief Overview
“Dietary Reference Intakes” (DRI) is an umbrella term for four reference values:
- Estimated Average Requirements (EAR)Average daily intake levels for nutrients estimated to meet the needs of 50 percent of the target group. Used in nutrition research and policy-making. EARs form the basis for which RDA values are set.
- Recommended Dietary Allowances (RDA)Based upon the EAR, these are nutrient-intake goals designed to meet the requirements of 97 to 98 percent of the target group for a given nutrient.
- Adequate Intakes (AI)If scientific data is insufficient to establish an EAR value, an AI is established based on the scientific data that is available. As with the RDA, the AI serves a nutrient-intake goal.
- Tolerable Upper Intake Levels (UL)The highest average daily nutrient-intake level at which a nutrient can be consumed before it poses a risk of toxicity.
The DRIs are not minimum or maximum nutritional requirements and are not intended to fit everybody. They are to be used as guides only for the majority of the healthy population.Deng, S., B. J. West, and C. J. Jensen. “A Quantitative Comparison of Phytochemical Components in Global Noni Fruits and Their Commercial Products.” Food Chemistry 122, no. 1 (September 1, 2010): 267–70. http://www.sciencedirect.com/science/article/pii/S0308814610001111.
DRIs are important not only to help the average person determine whether their intake of a particular nutrient is adequate, they are also used by health-care professionals and policy makers to determine nutritional recommendations for special groups of people who may need help reaching nutritional goals. This includes people who are participating in programs such as the Special Supplemental Food Program for Women, Infants, and Children. The DRI is not appropriate for people who are ill or malnourished, even if they were healthy previously.
The DRIs are inclusive of all four reference values.
© Networkgraphics
Determining Dietary Reference Intakes
Each DRI value is derived in a different way. See below for an explanation of how each is determined:
- Estimated Average Requirements. The EAR for a nutrient is determined by a committee of nutrition experts who review the scientific literature to determine a value that meets the requirements of 50 percent of people in their target group within a given life stage and for a particular sex. The requirements of half of the group will fall below the EAR and the other half will be above it. It is important to note that, for each nutrient, a specific bodily function is chosen as the criterion on which to base the EAR. For example, the EAR for calcium is set using a criterion of maximizing bone health. Thus, the EAR for calcium is set at a point that will meet the needs, with respect to bone health, of half of the population. EAR values become the scientific foundation upon which RDA values are set.
- Recommended Daily Allowances. Once the EAR of a nutrient has been established, the RDA can be mathematically determined. While the EAR is set at a point that meets the needs of half the population, RDA values are set to meet the needs of the vast majority (97 to 98 percent) of the target healthy population. It is important to note that RDAs are not the same thing as individual nutritional requirements. The actual nutrient needs of a given individual will be different than the RDA. However, since we know that 97 to 98 percent of the population’s needs are met by the RDA, we can assume that if a person is consuming the RDA of a given nutrient, they are most likely meeting their nutritional need for that nutrient. The important thing to remember is that the RDA is meant as a recommendation and meeting the RDA means it is very likely that you are meeting your actual requirement for that nutrient.
Understanding the Difference
There is a distinct difference between a requirement and a recommendation. For instance, the DRI for vitamin D is a recommended 600 international units each day. However, in order to find out your true personal requirements for vitamin D, a blood test is necessary. The blood test will provide an accurate reading from which a medical professional can gauge your required daily vitamin D amounts. This may be considerably more or less than the DRI, depending on what your level actually is.
- Adequate Intake. AIs are created for nutrients when there is insufficient consistent scientific evidence to set an EAR for the entire population. As with RDAs, AIs can be used as nutrient-intake goals for a given nutrient. For example, there has not been sufficient scientific research into the particular nutritional requirements for infants. Consequently, all of the DRI values for infants are AIs derived from nutrient values in human breast milk. For older babies and children, AI values are derived from human milk coupled with data on adults. The AI is meant for a healthy target group and is not meant to be sufficient for certain at-risk groups, such as premature infants.
- Tolerable Upper Intake Levels. The UL was established to help distinguish healthful and harmful nutrient intakes. Developed in part as a response to the growing usage of dietary supplements, ULs indicate the highest level of continuous intake of a particular nutrient that may be taken without causing health problems. When a nutrient does not have any known issue if taken in excessive doses, it is not assigned a UL. However, even when a nutrient does not have a UL it is not necessarily safe to consume in large amounts.
Figure 2.1 DRI Graph
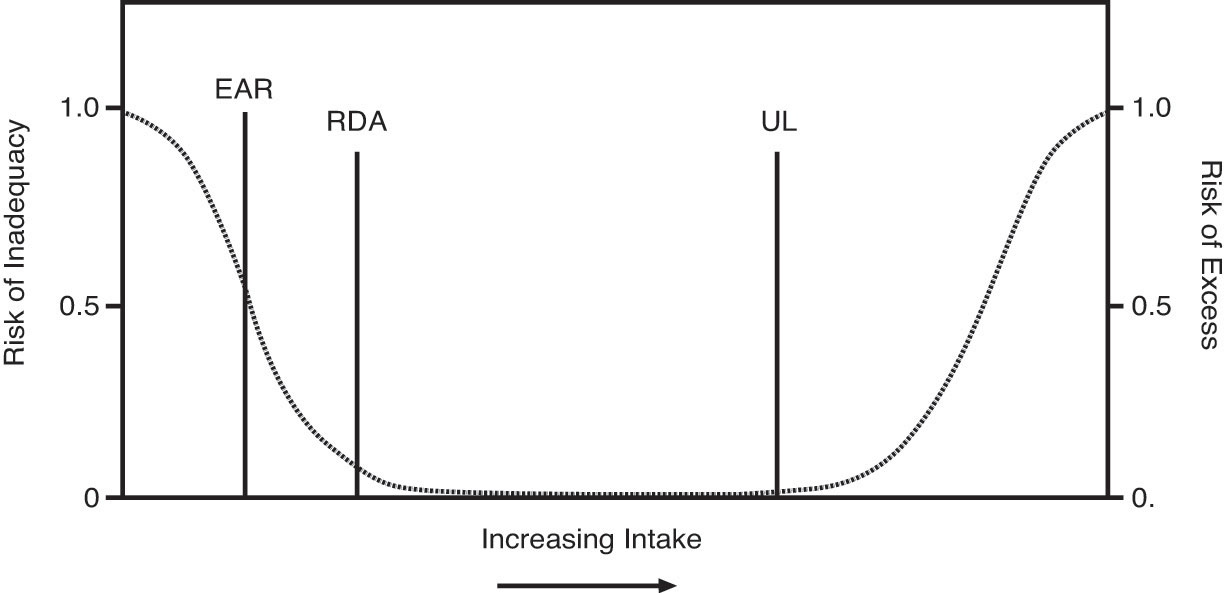
This graph illustrates the risks of nutrient inadequacy and nutrient excess as we move from a low intake of a nutrient to a high intake. Starting on the left side of the graph, you can see that when you have a very low intake of a nutrient, your risk of nutrient deficiency is high. As your nutrient intake increases, the chances that you will be deficient in that nutrient decrease. The point at which 50 percent of the population meets their nutrient need is the EAR, and the point at which 97 to 98 percent of the population meets their needs is the RDA. The UL is the highest level at which you can consume a nutrient without it being too much—as nutrient intake increases beyond the UL, the risk of health problems resulting from that nutrient increases.
Source: Institute of Medicine. © 2012 National Academy of Sciences. All Rights Reserved. http://www.iom.edu.
- Acceptable Macronutrient Distribution Ranges. The Acceptable Macronutrient Distribution Range (AMDR)The value of the energy-yielding nutrients carbohydrates, protein, and fat, expressed as percentages of total daily calorie intake, sufficient to provide total adequate energy needs; staying within the AMDR is associated with reducing the risks for developing chronic disease. is the calculated range of how much energy from carbohydrates, fats, and protein is recommended for a healthy diet. People who do not reach the AMDRs for their target group increase their risk of developing health complications. See Chapter 10 "Nutrients Important for Metabolism and Blood Function" for more information on calculating requirements.
Table 2.7 AMDR Values for Adults
| Nutrient | Value (percentage of Calories) |
|---|---|
| Fat | 20.0–35.0 |
| Carbohydrate | 45.0–65.0 |
| Protein | 10.0–35.0 |
| Polyunsaturated fatty acids | 5.0–10.0 |
| Linolenic acid | 0.6–1.2 |
Source: Food and Nutrition Board of the Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. (Washington, DC: National Academies Press, 2002).
Tips for Using the Dietary Reference Intakes to Plan Your Diet
You can use the DRIs to help assess and plan your diet. Keep in mind when evaluating your nutritional intake that the values established have been devised with an ample safety margin and should be used as guidance for optimal intakes. Also, the values are meant to assess and plan average intake over time; that is, you don’t need to meet these recommendations every single day—meeting them on average over several days is sufficient.
Key Takeaways
- Nutrient-intake recommendations set for healthy people living in the United States and Canada are known as Dietary Reference Intakes.
- The DRIs includes the AI, EAR, RDA, and UL for micronutrients and the AMDR ranges for energy-yielding macronutrients. The DRI provide a set of standards for researchers and government policy-makers, and specifies nutrient consumption guidelines for individuals.
Discussion Starter
- Why do you think it is important for the government to set the DRI standards? How will you use this information for your personal dietary choices?