This is “Supply and Demand in Health-Care Markets”, section 16.1 from the book Theory and Applications of Economics (v. 1.0). For details on it (including licensing), click here.
For more information on the source of this book, or why it is available for free, please see the project's home page. You can browse or download additional books there. To download a .zip file containing this book to use offline, simply click here.



16.1 Supply and Demand in Health-Care Markets
Learning Objectives
- What factors determine the price and quantity of health care?
- In what sense is spending on health an investment?
- What factors determine the demand for health-care services?
- What is the production function for health?
Suppose we want to explain why health care is more expensive in the United States than in Europe. Then supply and demand seems like a natural starting point. If we imagine a market for health care drawn in the usual way, with the quantity demanded on the horizontal axis and the price on the vertical axis, then the question becomes, “Why is the price of health care higher in the United States than in Europe?”
Supply and demand offers two possible answers (Figure 16.3 "Two Explanations for Why Health Care in the United States Is More Expensive Than in Europe"). The prices can be high because demand is high. For example, if the demand curve is further to the right in the United States compared to Europe (part [a] of Figure 16.3 "Two Explanations for Why Health Care in the United States Is More Expensive Than in Europe"), this implies—all else being equal—higher prices in the United States. The other reason for high prices is because supply is limited. If the supply curve in the United States lies further to the left than the supply curve in Europe (part [b] of Figure 16.3 "Two Explanations for Why Health Care in the United States Is More Expensive Than in Europe"), then this also would imply—all else being equal—higher prices for health care in the United States. Neither argument seems that compelling, which naturally leads us to wonder if the supply-and-demand framework is really the best framework for analyzing health care. In fact, there are good reasons to think that the supply-and-demand framework is not the best approach to this market.
Figure 16.3 Two Explanations for Why Health Care in the United States Is More Expensive Than in Europe
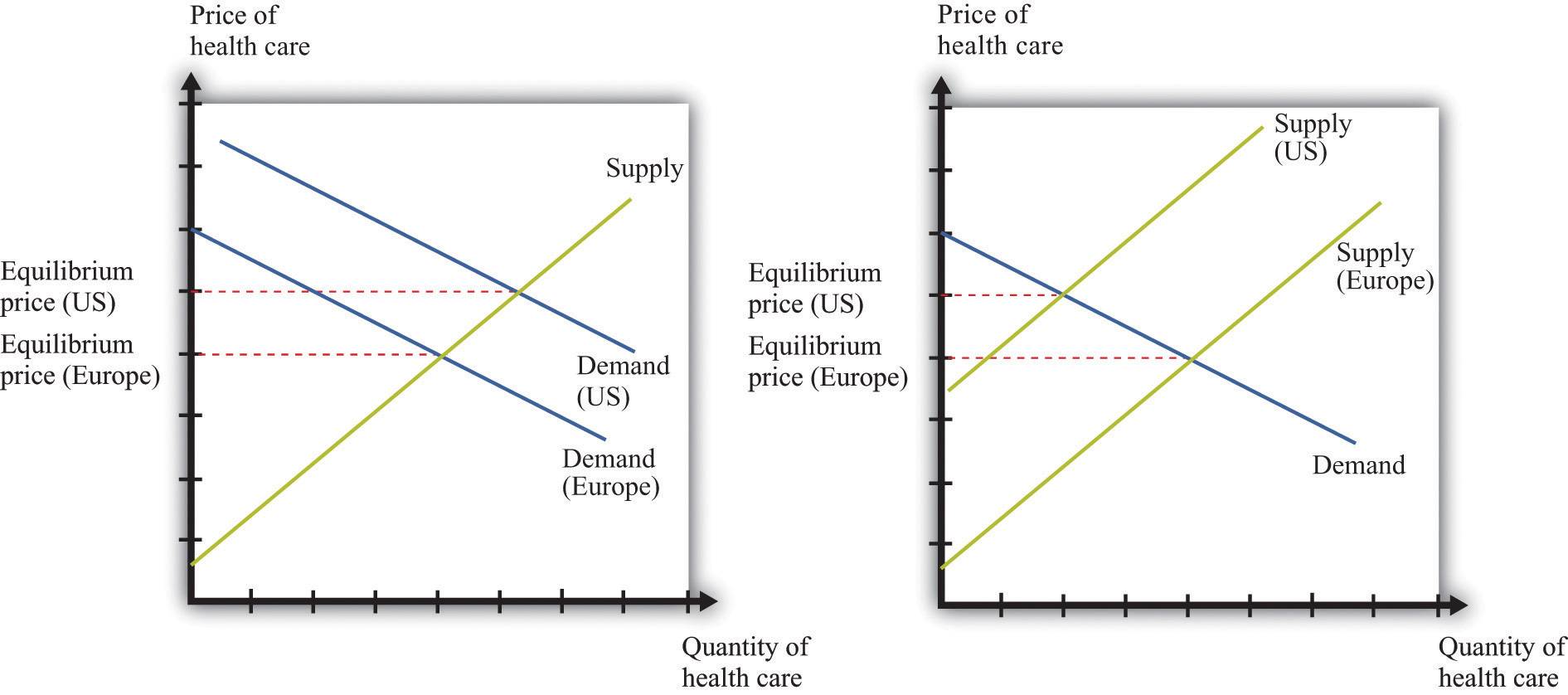
Supply and demand offers two possible explanations of high health-care costs in the United States: demand in the United States is high (a), or supply in the United States is limited (b). Neither is a very compelling explanation.
Let us think about the demand side first. Our standard approach to demand is based on the idea that each individual will consume a good or a service up to the point where the marginal valuationThe maximum amount an individual would be willing to pay to obtain one extra unit of that good. from one more unit equals the price of that additional unit.Chapter 4 "Everyday Decisions" explains this idea in more detail. Unfortunately, the health-care consumer often has very little idea of the value—let alone the marginal valuation—of the particular treatment being received. The consumer is very often not paying the full price for that treatment because the cost is frequently covered, at least in part, by insurance. Together, these mean that our traditional approach to demand does not work very well for health-care services.
The supply side is also problematic. First of all, some health-care suppliers have significant market powerA firm that has a downward-sloping demand curve.. This does not mean that we can get no insights from supply-and-demand reasoning. But it is trickier to compare the price of health care across countries because we have to consider differences in market power as well. A bigger problem is that some health-care suppliers, such as hospitals, are either government-controlled or not-for-profit institutions. The standard economic approach presumes that firms seek to make as much profit as possible, but government or not-for-profit hospitals may not have profit maximization as their goal.
In addition, health-care prices are not necessarily determined by supply and demand. Again, the government has a significant influence on prices: for example, the governments in some countries set prices for pharmaceutical products. Even if they are not set by the government, prices may be determined by bargaining between, say, hospitals and drug companies rather than by supply and demand. Furthermore, if people need health-care services, then their demand is likely to be very inelastic (the quantity demanded does not respond much to price changes). Inelastic demand is not, in and of itself, a problem for a competitive market. It just means that the equilibrium price could be very high. But if we couple inelastic demand with consumers who lack information and add in some market power by suppliers, then matters become more complicated. Perhaps you already have a sense of why: we have a large group of consumers with very inelastic demand who are relatively uninformed. This sounds like a gold mine for the supplier.
We have so far ignored the issue of what exactly is being traded in this market. “Health-care services” can mean many very different things:
- Labor time of various trained professionals, such as GPs, specialists, nurses, medical technicians, pharmacists, and many others
- Procedures and testing, such as magnetic resonance imaging (MRI) scans and laboratory analyses of blood samples
- Hospital and nursing care services
- Emergency services such as ambulances
- Pharmaceutical products (which itself covers a huge range, from bandages to chemotherapy drugs)
You can probably think of other components as well. So it is more than a little misleading to treat health care as something homogeneous that is bought and sold in a single market.
We hope that by now we have completely muddled your view of the health-care market. Our main point is that the simple framework of supply and demand is not sufficient for understanding health care. There are too many different markets, each with its own peculiarities and unusual features. And those features mean that there are several reasons why we might expect inefficiency. One, as we have already noted, is the presence of market power. Another is the various information problems we have mentioned. A third is that some aspects of health care have the characteristics of a public goodA good that is both nonrival and nonexcludable: it can be provided to many users without excluding anyone..
The Demand for Health Care
Now let us dig a little deeper into the demand side of health care.
Response to Price
The law of demand applies to health care as in other markets: as the price of health care increases, you demand less of it. But we must be careful. What matters is the price of health care to you. If you have health insurance, this price may be much lower than the actual cost of providing you with care. Under most health-insurance contracts, the marginal private cost of care to a household is less than the marginal social cost of providing that care. The household has an incentive to purchase a lot of health-care services because its purchases are, in effect, being subsidized by insurance companies. We take up the topic of health insurance later in this chapter.
Toolkit: Section 31.19 "Externalities and Public Goods"
You can review the distinction between marginal private cost and marginal social cost in the toolkit.
Another key characteristic of health care is that demand is relatively inelastic. If you are sick and require care, you will purchase health-care services at almost any price. Of course, your ability to purchase health care is ultimately limited by your income, but you are likely to trade off spending on many other products to purchase the medical care you need. This is why we often read stories about people without insurance being bankrupted by medical expenses.
Health as Investment
Everyone prefers being healthy to being sick. The demand for health care is in part an expression of this preference. One thing that makes health care different from most other goods and services, though, is that it is simultaneously an investment. Money you spend on being healthy today will also benefit you in the future. There are several different ways in which spending on health care represents an investment.
Mortality. One clear impact of our health-care choices can be seen in terms of mortality rates. Mortality rates measure how likely we are to die at different ages. In 2004, the mortality rate in the United States for people ages 15–24 was about 80 out of 100,000, or 0.08 percent. In contrast, the mortality rate for those over the age of 85 was 13,823 out of 100,000, or 13.8 percent.Mortality rates can be found at the National Center for Health Statistics, National Vital Statistics System, “Mortality Tables,” accessed March 14, 2011, http://www.cdc.gov/nchs/nvss/mortality_tables.htm. In other words, the typical young person has about a 1 in 10,000 chance of dying in a given year, whereas the typical old person has more than a 1 in 10 chance of dying.
It is not surprising that the mortality rate increases with age—that is, that young people have a lower probability of dying than older people. (Infants are an exception: a 6-month-old child is more likely to die than an 18-month-old child because very young children are particularly susceptible to certain diseases.) But these average mortality rates disguise a lot of variation, much of which is under our control. There are many behaviors that have predictable effects on our likelihood of dying. Smokers have a higher probability of dying than nonsmokers. Those who are obese have a higher probability of dying than those who are not. Diet, exercise, and risky behaviors (which includes everything from unprotected sex to skydiving) affect mortality rates as well.
Cigarette smoking is linked to lung cancer and thus to mortality. If you compare two similar individuals of the same age, one who is a smoker and the other a nonsmoker, then the mortality rate is significantly higher for the smoker. This does not mean that the smoker will necessarily die before the nonsmoker. It means that all else being the same, smoking increases the probabilityThe percentage chance that an outcome will occur. of death. Refraining from smoking is a type of investment in your future.
Our diet also affects our probability of becoming ill and of dying. As with cigarettes, there are often trade-offs between eating and drinking things we enjoy and the effects of such consumption on our long-term health. Making these types of choices is an economic decision. Each of us makes different choices because we value the taste of particular foods differently, and we value our overall health differently as well. If a thirty-year-old discovers he has elevated cholesterol levels that pose a long-term risk of heart disease, he may decide to adjust his diet, perhaps consuming less red meat. If an eighty-year-old learns the same news, he may not think the long-term benefit is worth giving up his steaks for.
Productivity. Being healthy also means that you can work and earn wages. One of the costs of poor health is lost days at work. This is a cost not only to the individual but also to society as a whole: the economy’s population is producing less output. If you are in poor health, then you risk losing wages for the days when you cannot come to work. Many employers provide insurance for these lost wages through the provision of sick days: if you are sick, you are not expected to work but you will still be compensated up to a contracted number of days per year. In addition, there is disability insurance as part of the social security system in the United States.The government program is summarized at http://www.ssa.gov/disability. Private employers sometimes also offer disability insurance as part of their compensation packages, and you can also purchase insurance directly from an insurance company.
Information Problems
Health care is an example of a good for which the typical individual is unable to determine the quality of what is being purchased. You can think of other examples, such as legal services and used cars. In such situations, how can we make good decisions? Generally we do so by relying on the advice of experts. In the case of health, these are the doctors, dentists, and other health professionals who are trained to analyze our health situation and make suggestions to us. We listen, try to understand, and, using their advice, make an informed choice.
Suppose you get a phone call from someone telling you they know of a stock, trading on Wall Street, that will double in price the following day. You might be very skeptical, suspecting that they have other reasons for wanting you to buy. Compare this to a conversation with a medical expert. Generally you are going to believe that the expert is acting in your best interests. Although you might get a second (or third) opinion, you do so because health problems are complex and the first expert may have missed something, not because you are afraid the doctor is misleading you in order to profit from your visit. But why do we trust medical experts so much more than the provider of stock tips? We generally do so because we trust that their incentives are aligned with our goals; that is, we hope that they are motivated to act in our best interests.
The Supply of Health Care
We now turn to the supply side of health care. Economists often talk of output being produced using a production function that uses labor, capital, and intermediate inputs. What is the production function of a hospital?
- The labor in a hospital includes doctors, surgeons, orderlies, technicians, nurses, administrative staff, janitors, and many others.
- The hospital buildings are part of the hospital’s capital stock. In addition, hospitals contain an immense quantity of other capital goods, such as hospital beds and diagnostic tools—everything from stethoscopes to x-ray machines.
- Intermediate inputs in a hospital include dressings for wounds, and pharmaceutical products, such as anesthetics used for operations.
Other sectors of the health-care industry likewise employ labor, capital, and intermediate inputs.
Toolkit: Section 31.17 "Production Function"
You can review the meaning and definition of a production function in the toolkit.
Doctors
If you look at the wall in your doctor’s office, you will typically see a large number of framed degrees and other qualifications. To become a doctor, you must first succeed as an undergraduate and then go through multiple years in medical school. After this comes an internship and then you finally graduate and can practice on your own. In most countries, you must have a license to practice medicine. This makes sense: you would not want anyone to advertise as a doctor regardless of their skill level. Most of us would be unable to tell whether a particular individual was a qualified professional or a quack. When buyers cannot easily evaluate the quality of the good or the service they are purchasing, it is useful to have external validations of quality.
Licensing provides more than a guarantee of quality, however. It also limits entry into the profession. Suppose you learned that a small group of lobbyists in your hometown wanted gas station owners to be licensed in the same way as physicians. You would quite rightly suspect that their goal was not to guarantee high-quality gasoline. More likely, they would be trying to limit the number of gas stations to increase their market power. Your suspicions would not be allayed if these lobbyists argued that gas was potentially a very harmful commodity, so by licensing the sellers of gas, they were protecting the community. In the case of doctors, the underlying reason for licensing is not so nefarious. But it still creates a barrier to entryA cost for new firms (or individuals) to enter into and compete in a market. that limits competition and increases market power, just as it would with gas stations.
Doctors differ from gas station owners in many other ways. Typically, we suppose that gas stations and other firms in an economy have profit maximization as a goal. It is this presumption that allows us to develop our theory of supply. Doctors not only think about profits but also take an oath of office, called the Hippocratic Oath, which is as follows:
I swear by Apollo, the healer, Asclepius, Hygieia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according to my ability and my judgment, the following Oath and agreement:
…
I will prescribe regimens for the good of my patients according to my ability and my judgment and never do harm to anyone…
I will not give a lethal drug to anyone if I am asked,…Wikipedia, s.v. “Hippocratic_Oath,” accessed March 14, 2011, http://en.wikipedia.org/wiki/Hippocratic_Oath.
This oath is administered to nearly everyone obtaining a medical degree.
Other Health-Care Workers
In addition to doctors and specialists, there are many other kinds of workers in the health care industry, including nurses, dental hygienists, administrative staff, technicians, staff in care facilities such as hospices and nursing homes, and many others. The health-care industry employs almost 10 percent of all civilian workers in the United States.
Table 16.1 "Employment in Health Services (in Millions)" shows the breakdown of employment by health-service site for three years: 2000, 2003, and 2006. We list some (not all) of the types of health sites. From the table, we see that the number of workers in this industry has increased from 12.2 million in 2000 to about 14.4 million in 2006. This increase is typical of many service industries and contrasts with manufacturing, where the number of workers employed is declining.
Table 16.1 Employment in Health Services (in Millions)
| Type of Health Service Site | 2000 | 2003 | 2006 |
|---|---|---|---|
| Physicians (offices and clinics) | 1.4 | 1.7 | 1.8 |
| Hospitals | 5.2 | 5.6 | 5.7 |
| Nursing care facilities | 1.6 | 1.9 | 1.8 |
| Total | 12.2 | 13.6 | 14.4 |
Source: National Center for Health Statistics, Health, United States, 2007 with Chartbook on Trends in the Health of Americans (Hyattsville, MD: US Department of Health and Human Services, 2007), table 105, accessed February 1, 2011, http://www.cdc.gov/nchs/data/hus/hus07.pdf.
Hospitals are the most important type of employment site for health-care workers. In 2006, 40 percent of health-care workers were employed in hospitals. About three-fourths of the workers in the health-care sector are women. Women are particularly prevalent in nursing care facilities: of the 1.6 million workers in nursing care facilities in 2000, about 1.4 million were women.
There is a wide variety of occupations within health care: managers, professionals (doctors, dentists, pharmacists, etc.), service occupations (assistants, cooks, cleaners, etc.), and office workers. Professional groups account for about 44 percent of all workers, while about 32 percent of the jobs are in service occupations. There will typically be considerable variation of wages within a sector because of the different occupations of workers in that sector. For example, individuals working in diagnostic laboratories earn, on average, close to twice the wage of workers in nursing homes.
Health-Care Capital
When we look at an industry such as health care, one way of describing it is by counting the number of doctors’ offices, clinics, and so on. There are many different kinds of establishments that provide health services. Hospitals are only one example; others include doctors’ offices, clinics, nursing homes, and so on. According to the Bureau of Labor Statistics (http://www.bls.gov/oco/cg/cgs035.htm), in 2008, there were 595,800 establishments in the health-care sector in the United States. Of these, doctors’ offices are 36 percent. Hospitals are only 1 percent.US Department of Labor, Bureau of Labor Statistics, “Career Guide to Industries, 2010–11 Edition: Healthcare,” accessed March 14, 2011, http://www.bls.gov/oco/cg/cgs035.htm. Another way to describe the industry is by detailing the number of workers employed in different activities, as in Table 16.1 "Employment in Health Services (in Millions)".
Taken together, these statistics paint an interesting picture. Hospitals are a small fraction of the total health-care establishments but employ 35 percent of the workers. This tells us that there are relatively few hospitals (compared to doctors’ offices), but they are big. About 70 percent of hospitals employ more than 1,000 workers. Such a pattern is not peculiar to the health-care sector. In US manufacturing, the majority of establishments are small, and a few large establishments employ the majority of workers.This is described in Steven J. Davis, John C. Haltiwanger, and Scott Schuh, Job Creation and Destruction (Boston, MA: MIT Press, 1998). We discuss this phenomenon in more detail in Chapter 9 "Growing Jobs".
The ownership of hospitals is also complicated. Some are private, while others are public, meaning that federal, state, or even county governments run them. In addition, not all private hospitals are in business for profit; some are classified as not-for-profit institutions. Table 16.2 "Hospital Activity, 2005" provides a breakdown of hospitals by type. From this table, you can see that most admissions are in not-for-profit hospitals that are not federally run. Their goal is largely to provide a public service. These hospitals have a length of patient stay averaging about 5.5 days.
Table 16.2 Hospital Activity, 2005
| Type of Hospital | Admissions (Thousands) | Average Length of Stay (Days) |
|---|---|---|
| All | 37,006 | 6.5 |
| Federal | 952 | 11.6 |
| Nonfederal, not-for-profit | 25,881 | 5.5 |
| Nonfederal, for-profit | 4,618 | 5.3 |
Source: National Center for Health Statistics, Health, United States, 2007 with Chartbook on Trends in the Health of Americans (Hyattsville, MD: US Department of Health and Human Services, 2007), table 105, accessed February 1, 2011, http://www.cdc.gov/nchs/data/hus/hus07.pdf.
There are other capital goods that enter the production function for the health sector. For example, pharmaceutical production facilities are part of this capital stock. So too is the capital stock of companies that produce the machines, such as MRIs, used in doctors’ offices and hospitals.
Technological Progress
Technological advances in health care are truly staggering. Technological progress in this sector, as in other sectors, comprises both product and process innovations. By product innovations, we mean increases in the types of goods and services available to households and doctors. A leading example is the vast array of drugs now available on the market, which is the outgrowth both of research and development at pharmaceutical companies and of publically funded research. Another example is the advanced machinery used in modern health-care facilities. A modern dentist’s office is filled with high-speed drills, x-ray machines, and other pieces of technology that would have been unthinkable in your grandparents’ day. MRI machines are another example: these are a significant advance over previous imaging techniques such as X-rays, but they are expensive—a new MRI machine will typically cost a hospital more than $1 million.An article describes this technique at NOVA, “The Picture Becomes Clear for Magnetic Resonance Imaging,” accessed March 15, 2011, http://www.science.org.au/nova/062/062key.htm.
Process innovations refer to how techniques are implemented. For example, surgeons today can perform operations that surgeons of previous generations could not even imagine. The knowledge for these procedures was created by a few people and then taught to others in medical school and other training programs.
Process and product innovations come together when you compare how certain procedures are performed now relative to years ago. Consider surgery to repair a hernia. The first hernia (hiatal) surgery took place around 1919, and the procedure was risky and painful. Even relatively recently, a procedure like this involved hospital stays, many days lost from work, and a significant risk of medical complications.For the history of hiatal hernia surgery, see Nicholas Stylopoulos and David W. Rattner, “The History of Hiatal Hernia Surgery: From Bowditch to Laparoscopy,” Annals of Surgery 241, no. 1 (2005): 185–193, accessed March 14, 2011, http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1356862. Today, the leading method for surgery uses a piece of capital called a laparoscope—a tube with light that allows a surgeon to see inside a patient’s abdominal cavity. Then, using another instrument, again inserted through a small incision, the surgeon can repair the hernia. Remarkably, this is an outpatient procedure. The patient emerges from the hospital with a few small wounds and can return to work and normal life within a few days.
Price Determination
If this chapter were like most others in this book, we would now turn to a discussion of how supply and demand interact in a competitive market to determine the price. Or, recognizing that firms with market power set prices, we might use the condition that marginal revenue equals marginal cost to talk about price determination. Unfortunately, when it comes to understanding the market for health care, these tools are not as useful.
To understand why, imagine you want to book a hotel room in New York City. You can call up any hotel and find the price of a room. Or you can go on the Internet and check prices either at the hotel’s website or at any number of other sites that provide booking services. You can find information about the hotel online, read reviews from previous guests, and talk to hotel staff members on the telephone if you need more information. If you are in the city, you can also walk into a hotel and find out the price and the hotel’s amenities.
Now compare this to a hospital. It is much harder to get information about prices, and you cannot simply walk in off the street and purchase an operation. You can in fact find out prices for hospital procedures if you look hard enough. For example, there is a website that allows you to find charges for different procedures in Wisconsin (http://www.wipricepoint.org). Here you can “shop” for, say, different types of knee surgery. But these charges do not necessarily reveal the true price to you as a consumer because they may not include all the costs of doctors and other inputs. If you have insurance coverage, meanwhile, you need to find out what portion of any bill will be covered by your insurance. Figuring out the price of a procedure is quite complicated.
How, then, are prices determined? And, importantly, what price are we talking about: the price you pay or the money received by the hospital? Many of the most important prices are determined by the interaction of a few big players, including the government, insurance companies, and pharmaceutical companies. Figure 16.4 "Payments to Hospitals and Doctors" gives a sense of the sources of income for hospitals and doctors. Hospitals and doctors get paid by insurance companies, households, and the government.
- Medicare (http://www.medicare.gov/default.aspx) is a federal program intended to provide health services to elderly (over 65) and disabled people. It covers nearly 40 million people. Under this program, the government sets fees for services provided by physicians. A listing of those fees is available through the Health and Human Services website.See Centers for Medicare and Medicaid Services, “Overview,” accessed March 14, 2011, http://www.cms.gov/apps/physician-fee-schedule/overview.aspx. A search engine at that site allows you to look for specific fees. These are the fees the government will pay physicians and hospitals for these services.
- Medicaid (http://www.cms.gov/MedicaidGenInfo) is run by the US government in conjunction with state governments.The states design the programs subject to approval by the federal government. Thus there are differences across states. The federal government reimburses states according to a rule that depends on the average income per person in that state. This program provides health care to low-income households through payments made directly to a health-care service provider, such as a hospital.
Figure 16.4 Payments to Hospitals and Doctors
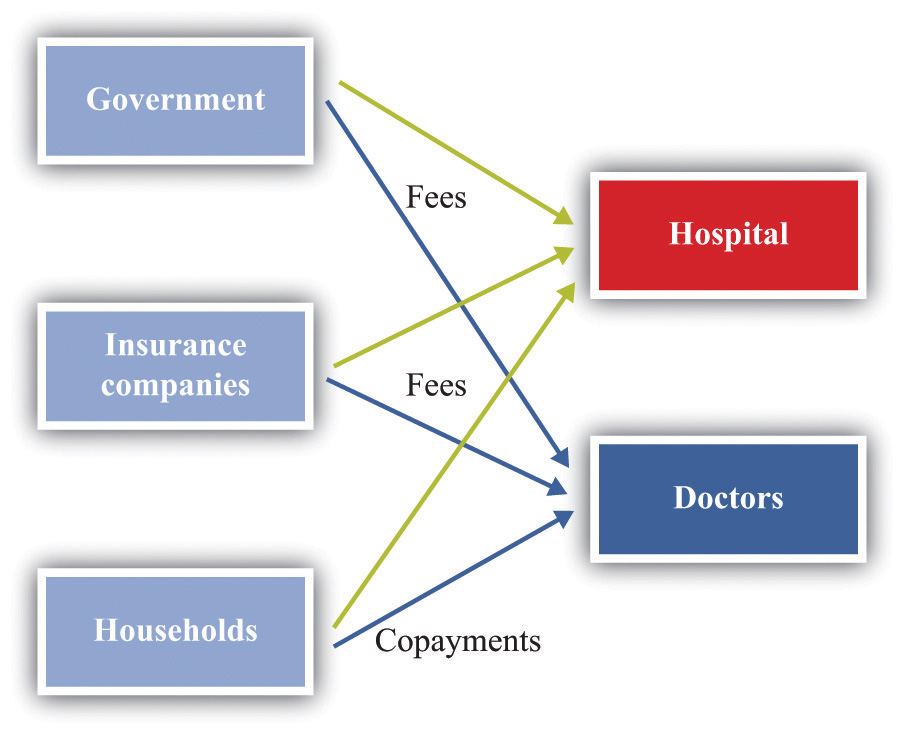
Because of these programs, the government is a big player in the health-care market. Government decisions determine the demand for health-care services. Governments do not take prices as given. In some cases, the government sets rates for certain procedures, and health-care providers respond. In other cases, the government is involved in negotiations—with pharmaceutical companies, for example.
Insurance companies provide additional sources of revenues to the hospital and a doctor. If you are a policyholder and are admitted to a hospital, your insurance company will reimburse the hospital for part of the cost of your care. It also reimburses your doctor directly. How much of that cost is reimbursed depends on your insurance policy. If you enter a hospital, say, for an operation, the amount of money the insurance company will pay the hospital is set by an existing agreement. As a result, hospital administrators face a complex set of repayment schedules. Reimbursement rates for a given service depend on who is buying the service, as the following quotation illustrates: “Medicaid pays 80 percent of what Medicare pays and about 50 percent of what a commercial insurance carrier like Blue Cross/Blue Shield pays. For example, if Medicaid reimbursed $500 for a gall bladder removal, Medicare would pay $625 and the commercial carrier $1,000 for the same procedure.”This quote comes from a hospital in Topeka, Kansas. See Jan Biles, “Medicare: Care versus Cost, cjonline.com, October 23, 2007, accessed February 1, 2011, http://www.cjonline.com/stories/102307/sta_211162036.shtml. Because of these differences in reimbursement rates, doctors and hospitals may sometimes decide not to provide services to certain patients. The same article notes that doctors sometimes turn down Medicaid patients because of these low rates.
And what will you pay if you walk into a hospital without health insurance? An April 28, 2008, article in the Wall Street Journal describes the plight of a cancer patient without adequate insurance. The patient was looking for treatment at a not-for-profit hospital in Texas. Her treatment required a payment of $105,000 in advance. This practice of requiring prepayment is part of a trend in the industry.
Hospitals are adopting a policy to improve their finances: making medical care contingent on upfront payments. Typically, hospitals have billed people after they receive care. But now, pointing to their burgeoning bad-debt and charity-care costs, hospitals are asking patients for money before they get treated.
Hospitals say they have turned to the practice because of a spike in patients who don’t pay their bills. Uncompensated care cost the hospital industry $31.2 billion in 2006, up 44 percent from $21.6 billion in 2000, according to the American Hospital Association.Barbara Martinez, “Cash before Chemo: Hospitals Get Tough. Wall Street Journal, April 28, 2008, A1.
Key Takeaways
- Due to informational problems for households, market power by suppliers, and government intervention, the market for health care cannot be analyzed by using standard supply-and-demand curves.
- Spending on health care today has an effect on your health status in the future. In that sense, this spending is an investment.
- The demand for health services, like other goods, depends on your income and the price of the services. Unlike your demand for many other goods, your demand for health services is influenced by the costs of health insurance. Also, unlike the case for many other goods, consumers who demand health services are relatively uninformed about the service they are buying.
- The production function for health takes inputs, such as doctors, nurses, and machines, and produces health-care services.
Checking Your Understanding
- List three reasons why the conventional supply-and-demand model may not fit the market for health services well.
- How is the demand for health services influenced by age?
- Give an example of two intermediate inputs into the provision of health-care services.